Awake despite an open skull: The complex surgery to save Ani’s five languages
A woman with a vascular malformation in her brain undergoes a peculiar medical intervention. While she is fully conscious, neurosurgeons map the language areas before removing the lesion to protect her vast linguistic skills

Between dreams, she wakes up. With her eyes open, feeling everything, Ani, 36, searches for friendly eyes among the crowd of healthcare workers. They come and go, moving around her in the neurosurgery operating room at the Hospital del Mar in Barcelona. ”Calm down, everything is fine,” a nurse whispers. “You’re doing very well, Ani!” exclaims Dr. Gloria Villalba, the neurosurgeon in charge of the intervention, as she injects anesthetic around the circumference of Ani’s skull. It’s not customary for a patient to be awake in the operating room, but in this case there’s no other choice. There are six hours to go with her skull open. Ani — who is completely lucid, only occasionally dozing — has to maintain her calm to assist the doctors. Without her help, problems could arise.
Ani has a cavernoma — a vascular malformation — lurking in a complex area of her brain, bordering the areas that control mobility and language. The injury has already caused dangerous bleeding in the brain, which may reoccur. The lesion must be removed, but it’s not easy to reach it. The patient speaks five languages and needs them for her work — hence, the neurosurgeons cannot even slightly damage any area that influences her language skills. To chart the safest path to the cavernoma, doctors need to map the brain regions around the lesion and find a point of access without impairing mobility or language. And only Ani can help them with this: the mapping and removal must be done while she is awake, as they perform neuropsychological tests to verify that there’s no brain damage in the process.
Ani’s native language is Armenian. All four of the others came to her through a mix of personal interest and life experiences. “Armenia is a small country, with a unique and ancient language… no one else speaks our language or understands our letters,” she notes. “So, I was interested in learning more languages to be able to communicate with others. ”She learned Russian — a legacy from when her country was part of the Soviet Union — at school. She also learned English, perfecting it with her taste for literature. Spanish, meanwhile, she cultivated from scratch when she moved to Spain 15 years ago. And, with her husband, she practiced French at home, as he’s a native speaker. She also honed it with a season in Quebec, Canada.
“Every place I went to, I wanted to know the language to learn the culture and understand [the local people’s] way of thinking. I was fascinated by learning each language,” she recounts. For this reason, the possibility of losing them — in addition to the impact it would have on her work — causes Ani to feel a deep “sadness.” But her life is at stake.

A cavernoma develops during childhood. This is a silent process, not necessarily giving off any signs or symptoms, the most common of which are bleeding in the brain and epileptic seizures. Ani’s injury showed up just a few years ago, in 2018, on a regular day at work. In the middle of a meeting, she began to mix up languages, couldn’t find the right words, lost her balance and fell down. Medical tests revealed that a kind of tangle of malformed veins and arteries in the left hemisphere of her brain — about one inch deep — was bleeding. In the process, this injury had altered some brain regions that control language and mobility. ”The problem [with the malformation] is that, once it has bled, the probability of it happening again is very high,” explains Dr. Villalba. This year, during a routine check-up, the doctors noticed that the lesion was already bigger and had started to bleed again. “The risk of a third [bleeding episode] was higher, so we opted to remove it. And now, I feel relieved, because they’ve done a huge amount of preparation… this gives me confidence that everything will turn out well,” Ani tells EL PAÍS, on the eve of the procedure.
Dr. Villalba admits that the injury is in a complex place and getting to it isn’t easy. Also, monitoring two or three languages has been done in the past, but five languages multiples the challenge. During the last team meeting outside the operating room, the neurosurgeon goes over the intervention again, noting the complexity. ”We don’t know if we’ll be able to remove the cavernoma. It leaves us very little leeway to get in. If we cannot access it, we’ll leave it as it is,” she says. The motto of the operation is to improve the situation or, in the worst case scenario, leave it be — never make it worse.
At stake are Ani’s five languages. And, in a way, her life as well. The threat of another hemorrhage — if the malformation is left in place — leaves little room for maneuver. After Dr. Villalba explains the situation to Ani, the patient feels two emotions overwhelm her: ”It [would make me] sad to stop speaking a language, but the most important thing is my life. I’m going to undergo very serious brain surgery… surgery that people undergo to save their lives. Mine could also be at stake. And, at the same time, I’m thinking about languages, but as something secondary. Although it would be rare that, from one day to the next, I would lose the ability to speak any.”
Ani clearly remembers a phrase by Dr. Villalba that determined her decision: “You have many years ahead of you and the cavernoma can give you problems. If you were my sister, I would tell you to have surgery.”

It’s after nine in the morning and Ani is already on the operating room table, halfway between sleep and wakefulness. Villalba begins to cut a straight line on the skin of her skull with the scalpel. Ani feels some pain and the anesthesiologist, Dr. Juan Fernández, increases the sedation until she falls asleep. For now, he notes, you don’t need to be fully awake. “This type of intervention is a challenge, because we have to keep the patient — especially at certain times — fully conscious. It’s important to talk a lot with her, to explain to her what the procedure consists of and when we’re going to require her full awareness. You also have to apply a good local anesthetic, which will allow us, at times when we cannot use sedation, to be able to hold her head in place so that it doesn’t move. The third important thing is sedation — with individualized adjusted doses — so that she can be unconscious, but still breathing on her own, at times when she’s not required to be awake,” Fernández explains. The drugs they use, analgesics and hypnotics, are fast-acting, in order to quickly regulate the level of consciousness.
The neurosurgeon reaches the wall of the skull, at the level of the left frontal and temporal lobe. She starts the craniotomy. With an electric drill, Villalba draws a circle on the skull and lifts it up, like a small lid. The sinuous grooves of the brain come into view and Ani begins to regain consciousness. The neurosurgeon asks for silence in the operating room to hear the patient. Now, it’s her turn.
Ani’s participation is key to mapping the five languages, Villalba emphasizes. “We’ll do a series of tests, because language isn’t just speaking: it’s also understanding, naming and describing. We’ll do the tests for five languages and, in addition, another test for facial expression recognition. This is to validate social cognition — which is something that has barely been studied — especially in the left hemisphere [of the brain],” Villalaba explains. The doctors will use the opportunity to see if there are critical areas for emotional processing on that side of the brain as well.
Flags of different countries and facial icons are placed on the table of surgical instruments. Borja Lavín, the scrub nurse, precisely cuts out each illustration, while Villalba grips a pointed stimulator, with which she will apply small discharges in the patient’s cerebral cortex. The sparks — applied to a specific area of the brain — will cause certain neuronal systems that are related to language or mobilily to stop working. When that happens, the neurosurgeon will mark that point with a sticker — she will know that the area is compromised and she will not be able to go there during the surgery. The doctors begin to measure Ani’s mobility with tiny electrical lashes to that exposed piece of brain. Nothing happens… until it happens. At one point, Ani complains that her mouth has gone numb and Villalba plants a tiny pennant with a pair of thick lips drawn between two grooves in the brain. Then another. And one more.
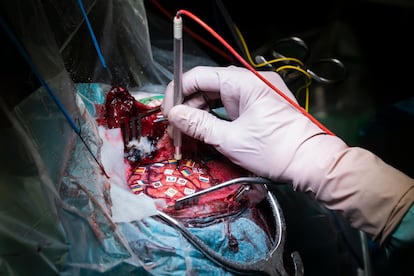
The patient continues with the test, counting from one to 10 in Spanish over and over again. She chants numbers and describes everyday objects that pop out of a computer screen, as she relentlessly raises and lowers her arm until, suddenly, as if by magic, her body stops. The patient’s forearm is suspended in the air and words do not come out of her mouth. The doctor has just stimulated a risk area and fixed a Spanish flag at a point on the frontal lobe. “I know the word, but it doesn’t come out,” Ani says. The mapping continues, in Armenian, English, French and Russian. Sometimes, Ani’s arm freezes again and her voice stops. “I knew what it was, but I couldn’t find the word,” she insists. At times, during the test of emotions, she also fails. Sometimes she isn’t able to correctly identify whether the expression of a face is happy, lazy, sad, or angry.
After two hours of exercises, the visible portion of her brain is full of colorful flags. There is barely a free hole to the right, with only a tiny window that is less than one-fifth of an inch through which the brain can be penetrated so the cavernoma can be extracted. Villalba hesitates, argues with her team, weighing the possibilities. The margin is minimal. “In the study we do to prepare for surgery, we study motor and language functions — it gives us an idea of how we can see neurons in surgery. But it’s only a projection. The information told us that it was possible to access the cavernoma in a viable way… but, with intraoperative monitoring, we’ve found a slightly more complex situation: as there’s a wide distribution of the five languages [in her brain], this allows us very little space to access [the lesion],” she states.
With the help of a surgical microscope, Villalba begins to penetrate the brain in search of the vascular malformation. Ani continues with the tests: the mapping is complete, but it’s important to check that the mobility and language functions are still intact as the doctors make their way through the brain. In the background, a vascular ball appears on screen. The neurosurgeon extracts it little by little, without looking up.

Villalba manages to remove the entire cavernoma, which rests, frayed and tiny, in a small container. It’s not without a cost. Everything that could have been complicated has really been complicated, the neurosurgeon admits. “The space we had to access the cavernoma was very small. The surgery has challenged us, but we’ve been able to do it. Once we’ve reached the lesion, the ideal is to be able to remove it en bloc, in one piece, to make sure that you remove every last millimeter… but since this cavernoma had previously bled, it was totally stuck to the brain and we had to take it out little by little,” she explains. Until the control MRI, in a few days, the team will not know if they have removed 100% of the cavernoma. It’s already after 3 p.m. when the neurosurgeons — who have already closed the craniotomy — are busy sewing up the last layers of skin. Ani is now resting under the effects of sedation. Despite the difficulties, the doctors are optimistic. “When we finished monitoring and resecting the cavernoma, the patient [moved well] and spoke correctly. We’re happy with how the surgery has gone,” Villalba states.
A month after that very long morning in the operating room, Ani is recovering by leaps and bounds. Her five languages are intact. In subsequent MRIs, there is no trace of the cavernoma or unwanted side effects. She lacks some agility in her speech, but she’s happy: “I have to plan what I’m going to say… that takes a lot of effort. Maybe I don’t speak as fluently as before, but it’s a matter of time. In a month or two, I think I’ll recover everything,” she notes.
Ani looks back and remembers the long road that she has travelled. It was hard, both physically and emotionally. The first hemorrhage happened when her eldest son was barely 10 months old. The intervention took place when the younger one was only seven months old. “An interrupted maternity,” she sighs, due to “the restlessness and anguish” of living with a constant threat. She is still recovering from that sense of regret.
“It was a strange feeling when I went home after the operation. I saw my children… [they looked] very big. And the feeling of being able to hug them was like something new, as if I had never done it before. That interrupted maternity is a process. Emotionally, it hasn’t been easy.” At least, she says, the most important thing is that it’s all over: the dangerous malformation, along with the uncertainty that came from living with it.
Sign up for our weekly newsletter to get more English-language news coverage from EL PAÍS USA Edition









































